 |
Case Report
Triple ectopic thyroid: A rarely described entity
1 Resident Physician, Department of Medicine, Case Western Reserve University/University Hospitals Cleveland Medical Center, Cleveland, Ohio, USA
2 Assistant Professor of Medicine, Department of Medicine, Case Western Reserve University School of Medicine/Louis Stokes VA Medical Center, Cleveland, Ohio, USA
3 Service Chief, Nuclear Medicine Service, VA Northeast Ohio Healthcare System, Cleveland, Ohio, USA
Address correspondence to:
Stephanie AC Pitts
MD, 1717 E 9th St, Suite 1805, Cleveland, OH 44114,
USA
Message to Corresponding Author
Article ID: 100067Z09SP2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Pitts SAC, Sood P, Derrwaldt RD. Triple ectopic thyroid: A rarely described entity. J Case Rep Images Med 2022;8(1):5–9ABSTRACT
Introduction: Triple ectopic thyroid is a rarely described entity with only eight previous cases reported in the literature. This case is the first-described discovery of triple ectopic thyroid in a middle-aged male.
Case Report: A 46-year-old male with a past medical history of hypothyroidism and cannabis use disorder presented to his primary care physician with a globus sensation and left cervical lymphadenopathy for two weeks. A computed tomography (CT) scan of the neck with contrast identified three high attenuation areas: the first in the midline floor of the mouth extending posteriorly to the base of the tongue, the second at the base of the tongue, and the third in the midline of the neck just beneath the hyoid bone. Thyroid tissue was not identified in the orthotopic location. A follow-up thyroid uptake and scan confirmed that each of these high attenuation areas was also iodine avid, consistent with thyroid tissue.
Conclusion: The few cases of triple ectopic thyroid have mainly been discovered in female children with the most commonly described locations being the lingual (88%) and suprahyoid (88%) regions. Most patients were symptomatic with midline neck swelling. Overall, we describe the first case of triple ectopic thyroid in a middle-aged male and the first patient with ectopic thyroid located in the midline mouth.
Keywords: Computed tomography of thyroid anomalies, Hypothyroidism, Lingual thyroid, Thyroid anomalies, Thyroid diseases, Thyroid dysgenesis, Thyroid gland ectopic thyroid, Thyroid uptake and scan of thyroid anomalies, Triple ectopic thyroid
Introduction
During embryogenesis, the thyroid originates from the foramen cecum at the base of the tongue and finishes migrating toward its pre-tracheal position by the seventh week of gestation. This embryological process can arrest at any point, resulting in ectopic thyroid tissue. Generally, if ectopic thyroid tissue is present, there is only one ectopic site, rarely two. Exceedingly rare, with only eight cases reported in the literature, is triple ectopic thyroid [1],[2],[3],[4],[5],[6],[7],[8]. The cases previously reported in the literature were mainly discovered in female children. In this case report and literature review, we present an extremely rare case of triple ectopic thyroid in a middle-aged male.
Case Report
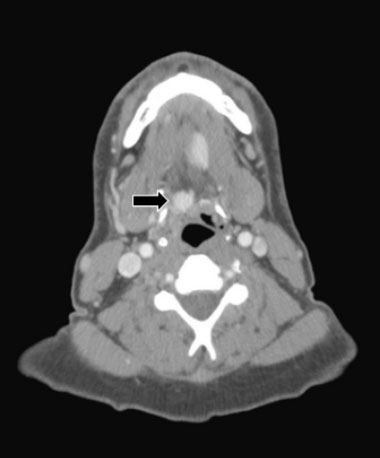
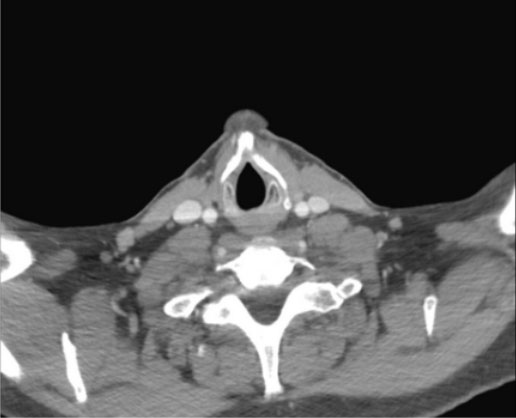
A 46-year-old male with a past medical history of hypothyroidism and cannabis use disorder presented to his primary care physician with a globus sensation and left cervical lymphadenopathy for two weeks. A computed tomography (CT) scan of the neck with contrast identified three high attenuation areas: the first in the midline floor of the mouth extending posteriorly to the base of the tongue (1.5 × 2.2 cm) (Figure 1), the second at the base of the tongue (1.4 × 1.8 × 3.0 cm) (Figure 2), and the third in the midline of the neck just beneath the hyoid bone (1.3 cm) (Figure 3). Thyroid tissue was not identified in the orthotopic location (Figure 4). A follow-up thyroid uptake and scan confirmed that each of these high attenuation areas was also iodine avid, consistent with thyroid tissue (Figure 5). Notably, there was no uptake in the normal orthotopic thyroid location.
In regard to the patient’s symptoms, he was diagnosed 12 years prior to presentation on routine screening and has been prescribed an increasing dose of levothyroxine replacement therapy since then. He did not have any thyroid imaging done at the time of diagnosis.
In regards to the patient’s symptoms, his left cervical lymphadenopathy and globus sensation were evaluated and not thought to be related to the ectopic thyroid tissue.



Discussion
Thyroid tissue originates from the foramen cecum at the base of the tongue during embryogenesis. As the endodermal cells proliferate, the thyroid diverticulum is created which begins migrating toward its pre-tracheal position [9]. The thyroid reaches its normal anatomic location by the seventh week of gestation [9]. The thyroglossal duct remains along the thyroid’s tract of descent until week ten of gestation when it degenerates [9]. This embryological process can arrest at any point resulting in ectopic thyroid tissue. The prevalence of ectopic thyroid tissue is approximately 1 per 100,000–300,000 people, though the prevalence increases dramatically to nearly 7–10% of the population when looking at autopsy studies [10]. The most common location for ectopic thyroid tissue is the foramen cecum (lingual ectopic thyroid) which comprises 90% of ectopic thyroid cases [10]. Other less common locations have been reported, mainly along the tract of the thyroglossal duct, including submandibular, suprahyoid, and infrahyoid [10]. Ectopic thyroid tissue has also been reported in areas inferior to the normal orthotopic thyroid location including intrathoracic (mediastinum, lung, and heart), struma ovarii, adrenal gland, duodenum, pancreas, and intestines [10]. In cases of dual ectopic thyroid tissue, the areas involved most commonly included the lingual and subhyoid sites [10].
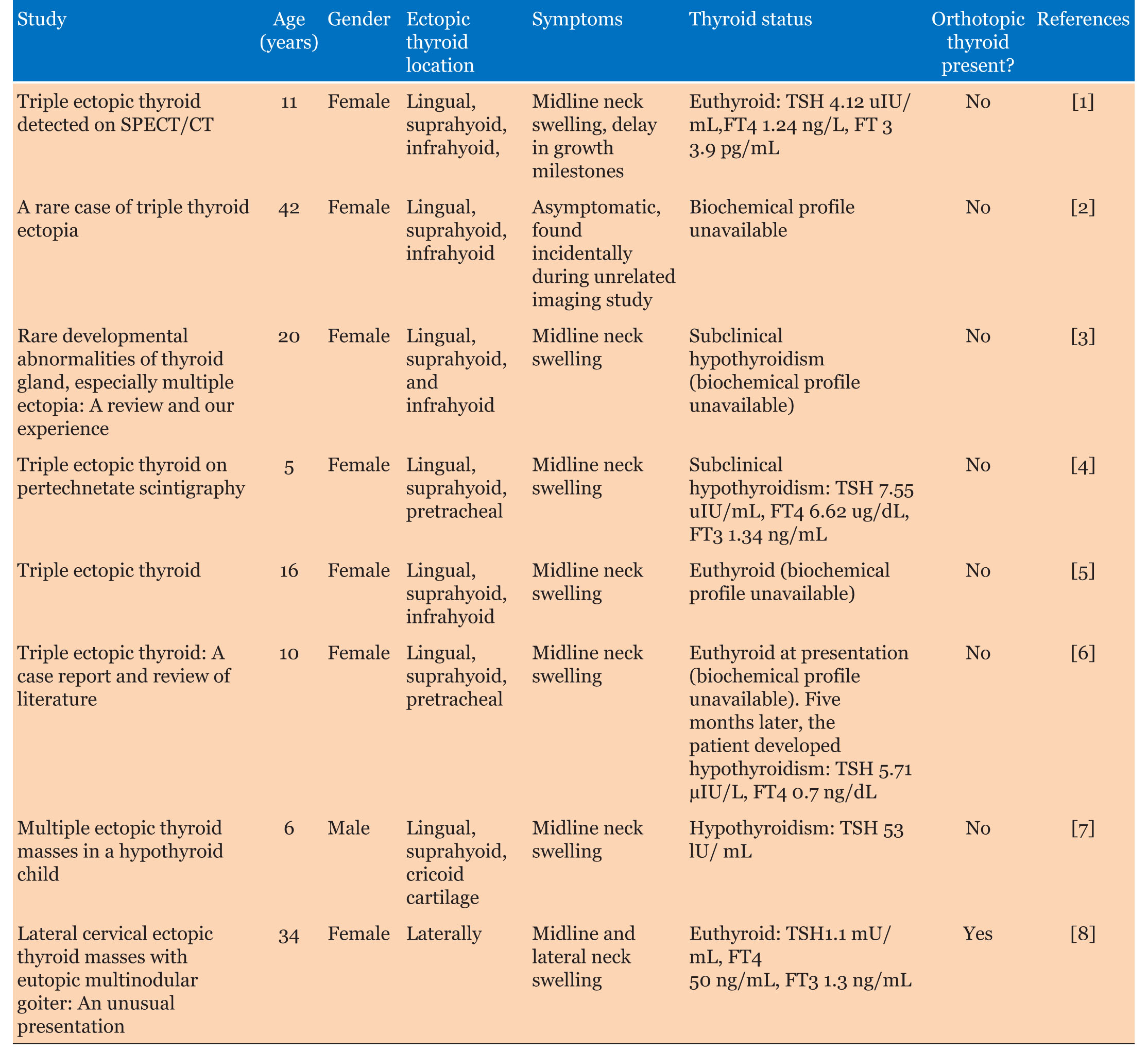
Even rarer than dual ectopic thyroid is triple ectopic thyroid. In fact, there are only eight previously reported cases in the literature [1],[2],[3],[4],[5],[6],[7],[8]. Here, we will review the previously reported cases including the most common location of the ectopic thyroid tissue as well as the age, sex, symptomatology, and thyroid function of each of these patients. This is also summarized in Table 1.
In the reported cases of triple ectopic thyroid, the most common locations were the lingual (88%) and suprahyoid (88%) regions [1],[2],[3],[4],[5],[6],[7]. Less common locations included the infrahyoid (50%), pre-tracheal (25%), and cricoid cartilage (13%) areas [1],[2],[3],[4],[5],[6],[7]. Lastly, one patient only had ectopic thyroid lateral to the orthotopic thyroid [8]. In addition to lingual (Figure 1) and infrahyoid (Figure 2) areas, our patient had ectopic thyroid in the midline mouth (Figure 3) which has not previously been described and would seem quite unusual given the embryological pathway in normal thyroid development.
In terms of age, the known cases of triple ectopic thyroid ranged from 5 years old to 42 years old [1],[2],[3],[4],[5],[6],[7],[8]. The average age was 18 years old. In terms of sex, seven of the eight known cases occurred in females [1],[2],[3],[4],[5],[6],[8]. The one previous male patient with triple ectopic thyroid was 6 years old at the time of diagnosis [7]. Therefore, our patient is not only the oldest described patient with triple ectopic thyroid at age 46, but he is also only the second described male patient and first described adult male patient.
In terms of symptomatology, 87.5% (seven out of eight) patients experienced neck swelling, mainly midline [1],[3],[4],[5],[6],[7],[8]. The last remaining patient was identified incidentally due to another imaging study [2]. Our patient experienced midline neck swelling which is likely related to the ectopic thyroid tissue. The globus sensation is thought to be unrelated to the ectopic thyroid tissue.
Finally, there was variation in the thyroid function of each of these patients at diagnosis. There was no information on the thyroid function status of one patient [2]. Of the remaining seven patients, three were euthyroid, two had subclinical hypothyroidism, one was hypothyroid, and the remaining patient was euthyroid upon diagnosis and subsequently developed hypothyroidism within five months of diagnosis [1],[3],[4],[5],[6],[7],[8]. Of note, only one patient had orthotopic thyroid tissue and she was euthyroid [8]. Our patient was hypothyroid and had been treated with increasing doses of levothyroxine for 11 years prior to diagnosis with triple ectopic thyroid. Given the early age of diagnosis of most of these patients, it is unclear at this time if hypothyroidism is perhaps a common manifestation of triple ectopic thyroid as these patients age.
Conclusion
All in all, triple ectopic thyroid remains an exceedingly rare diagnosis. Our patient is currently the only adult male patient described in the literature and the first patient with ectopic thyroid located in the midline mouth.
REFERENCES
1.
Agrawal K, Patro PSS, Pradhan P. Triple ectopic thyroid detected on SPECT/CT: A rare case report. Clin Nucl Med 2019;44(7):e453–5. [CrossRef]
[Pubmed]

2.
Rahalkar M, Rahalkar A, Solav S. A rare case of triple thyroid ectopia. Indian J Endocrinol Metab 2014;18(2):238–40. [CrossRef]
[Pubmed]
3.
Jain A, Pathak S. Rare developmental abnormalities of thyroid gland, especially multiple ectopia: A review and our experience. Indian J Nucl Med 2010;25(4):143–6. [CrossRef]
[Pubmed]
4.
Passah A, Arora S, Damle NA, Sharma R. Triple ectopic thyroid on pertechnetate scintigraphy. Indian J Endocrinol Metab 2018;22(5):712–3. [CrossRef]
[Pubmed]
5.
Konde SR, Singh H Retd, Pawar A, Sasane A. Triple ectopic thyroid. Med J Armed Forces India 2012;68(2):173–5. [CrossRef]
[Pubmed]
6.
Kuramoto R, Oikawa K, Fujita K, Oridate N, Fukuda S. Triple ectopic thyroid: A case report and review of literature. J Thyroid Disorders Ther 2013;2(2):126.
7.
Barai S, Bandopadhayaya GP, Kumar R, Malhotra A, Halanaik D. Multiple ectopic thyroid masses in a hypothyroid child. Pediatr Radiol 2004;34(7):584. [CrossRef]
[Pubmed]
8.
Nasiru Akanmu I, Mobolaji Adewale O. Lateral cervical ectopic thyroid masses with eutopic multinodular goiter: An unusual presentation. Hormones (Athens) 2009;8(2):150–3. [CrossRef]
[Pubmed]
9.
Arrangoiz R, Cordera F, Caba D, Muñoz M, Moreno E, de León EL. Comprehensive review of thyroid embryology, anatomy, histology, and physiology for surgeons. International Journal of Otolaryngology and Head & Neck Surgery 2018;7(4):160–88.
10.
Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: Anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol 2011;165(3):375–82. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Stephanie AC Pitts - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Pratima Sood - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ronnie D Derrwaldt - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Stephanie AC Pitts et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}